Chairman Gray and other members of the Council, thank you for the opportunity to submit this testimony. My name is Kate Coventry, and I am a Senior Policy Analyst at the DC Fiscal Policy Institute. DCFPI is a nonprofit organization that promotes budget choices to address DC’s economic and racial inequities and to build widespread prosperity in the District of Columbia, through independent research and policy recommendations.
I am here today to encourage the Council to use the recently identified unspent funds in the DC Healthcare Finance FY 2020 budget to strengthen the DC Healthcare Alliance. The Alliance is a program that provides critical health care coverage to residents with low incomes who do not qualify for Medicaid, most of whom are immigrants. Healthcare is a human right and truly vital during the current COVID-19 pandemic. The District should be doing all it can to ensure that as many residents as possible have access to insurance and that access is as easy as possible. DC should do this by removing onerous recertification requirements in the Healthcare Alliance.
Given their shared purpose, the DC Healthcare Alliance and Medicaid program should have identical, low-barrier application and recertification requirements. But the DC Healthcare Alliance requires participants to recertify every 6 months and does not allow participants to do this online while Medicaid only requires annual recertification and allows participants to do so online. These barriers contribute to both poor health outcomes and unnecessarily high program costs. [1]
We thank the administration for ensuring that no one loses eligibility during the public health crisis by temporarily waiving the in-person interview requirement for the Alliance, but we need permanent changes to Alliance application and recertification procedures to build a just recovery.
Shortened Eligibility Period Has Led to Turnover, Poorer Health, and Higher Costs
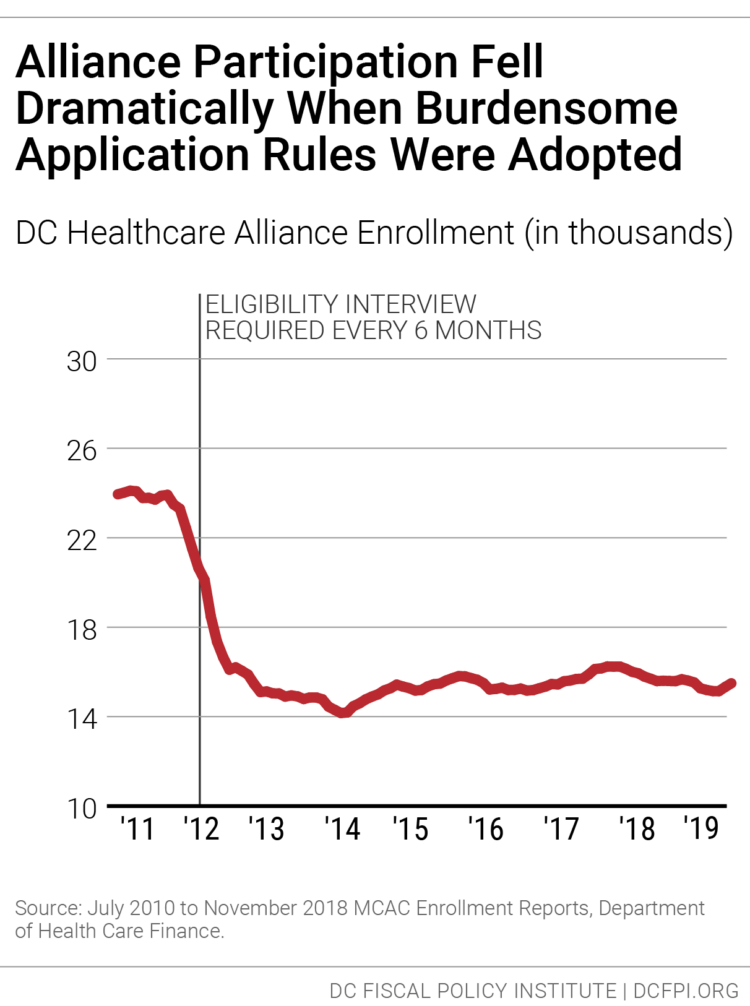
In 2011, DC implemented restrictive procedures residents had to follow to maintain their Alliance eligibility, including in-person interviews every six months, whereas Medicaid only requires annual recertification and no in-person interviews. The change in Alliance immediately led to a sharp drop in participation (Figure 1). Today, thousands of residents who should have health insurance do not, and the uninsured rate is much higher among Latinx DC residents [2] than others.
The restrictive rules also contribute to a high rate of turnover in the Alliance, as residents join the program but then drop off, due to the time-intensive requirements. Only 55 percent of Alliance participants renew their eligibility when it comes up, data from the District’s Department of Health Care Finance show.[3] Given that many Alliance members are working at jobs without paid leave and that visiting a Department of Human Services center can take an entire day or longer, it is not surprising that many are not able to renew their benefits.
This lack of continuous coverage contributes to poor health outcomes and high costs per person in the Alliance. Churn from frequent recertification increases health program costs because it limits access to preventive care, which means participants often are sicker when they re-enroll, and because sicker residents are most willing to go through the process of maintaining coverage. Healthcare Alliance costs have doubled in the past four years, even though participation has not grown. The cost increases appear to reflect other factors, including a growing number of older participants.[4]
The six-month recertification requirement also creates problems for other residents seeking public benefits. Data collected in 2015 suggest that Alliance recipients make up one-fourth of service center traffic in a given month, even though they represent a very small portion of service center clients.[5]
It is worth noting that DHCF director Turnage and senior staff met several times over the past year with DCFPI and other advocates to discuss this issue, and we appreciate their openness. DHCF staff also engaged in some analysis of Alliance participants, and in my opinion, the research did not point to widespread fraud. This is important given that concern over possible fraud is the primary argument made by DHCF for keeping the current 6-month recertification rule.
- For example, there is concern that some non-residents use a fake DC address to apply for the Alliance, and that in some cases, many people use the same address. But DHCF’s analysis found that only 6 percent of Alliance participants are in homes with five or more Alliance participants.
- DHCF also compared participants who cycled on and off with those that cycle off and do not return—with the possibility that some of those who don’t return may have been on the Alliance fraudulently. But DHCF found the characteristics of those who cycled off permanently to be roughly the same as those who cycle off and on. For example, roughly the same share in both groups had a connection to a non-DC address. The similarity suggests that people who cycle off permanently may be eligible but simply discouraged from remaining on the Alliance by burdensome rules.
The District Should Use Unspent Funds to Improve the Alliance
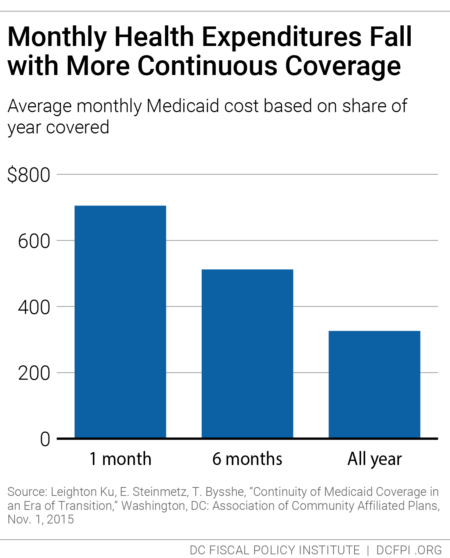
The $28.2 million in underspending in the FY 2020 budget that was recently identified as a source of funding for the Metropolitan Police Department is an opportunity to make the Alliance a more effective health care program—and to improve health outcomes for DC’s immigrants. Research from Medicaid, for example, shows that average health care costs go down the longer participants have coverage (Figure 2). DCFPI recommends the agency look at recipients who normally would have cycled off the Alliance but did not because of the waiver of the recertification requirement during the public health crisis to see how the longer coverage affected their health and health care costs.
The DC Council adopted legislation to remove the six-month requirement, but it has not gone into effect because the Mayor and Council have not identified the funding needed to serve the thousands of additional residents expected to receive coverage.
DC has been a leader in expanding health insurance coverage to improve resident health and reduce health disparities. Eliminating barriers to care is a critical component of those important city goals and would go a long way towards affirming support for our immigrant neighbors. This is particularly important now as Latinx residents have the highest incidence of coronavirus infection per capita in the District, at 1,200 per 100,000 people compared to 820 and 175 per 100,000 people for Black and white residents respectively.[6] These residents need health insurance so they can receive the care they need.
Thank you for the chance to submit this testimony.
[1] Ed Lazere, “No Way to Run a Healthcare Program: DC’s Access Barriers for Immigrants Contribute to Poor Outcomes and Higher Costs,” DC Fiscal Policy Institute, revised March 17, 2019, https://www.dcfpi.org/all/no-way-to-run-a-healthcare-program-dcs-access-barriers-for-immigrants-contribute-to-poor-outcomes-and-higher-costs/
[2] Jodi Kwarciany, “DC Has Disparities in Health Coverage Despite Its Low Uninsured Rate,” DC Fiscal Policy Institute, revised September 25, 2017, https://www.dcfpi.org/all/dc-disparities-health-coverage-despite-low-uninsured-rate/
[3] Ed Lazere
[4] Ibid
[5] Wes Rivers, DC Fiscal Policy Institute, and Chelsea Sharon, Legal Aid Society of the District of Columbia, “Testimony for Public Oversight Hearing on the Performance of the Economic Security Administration of the Department of Human Services District of Columbia Council Committee on Health and Human Services,” revised March 12, 2015, https://www.legalaiddc.org/wp-content/uploads/2015/03/CSharon3.12.15.pdf
6] Natalie Delgadillo, “Why Do Latinos Have The Highest Rate of Coronavirus Infection in D.C.?,” Dcist, May 11, 2020, https://dcist.com/story/20/05/11/why-do-latinos-have-the-highest-rate-of-coronavirus-infection-in-d-c/